
VentWorld Case Studies
MANAGEMENT OF PERSISTENT HYPERTENSION OF PERSISTENT HYPERTENSION IN THE NEWBORN USING HIGH FREQUENCY OSCILLATION
Published March 13, 2001
 |
Joseph D. Limauro M.Ed., R.R.T.
Dartmouth Hitchcock Medical Center Lebanon, NH
www.hitchcock.org/pages/resp2/resphome2.html
Contents (click to jump directly to that section, or scroll down to read the case)
INTRODUCTION
A 38 week newborn was delivered via elective c-section. The infant was large for gestational age weighing 4.0 kg and presented with cyanosis and significant respiratory distress including tachypnia, retractions, nasal flaring and poor oxygenation. The infant required manual ventilation with CPAP via ambu bag. SpO2 remained less than 85% on 100% oxygen. The initial chest x-ray suggested Respiratory Distress Syndrome. There was no maternal history to suggest pneumonia.
CASE PRESENTATION
|
The infant was intubated and given surfactant. Initial ventilator settings were: Pressure Control Mode, rate 40, PIP 26 cmH2O, FiO2 1.00, and PEEP 5 cmH2O.The ABG with these settings was pH 7.43, PCO2 37 mmHg and PO2 58 mmHg.
The infant continued to worsen over the next 4 hours. Ventilator settings were now: Pressure Control Mode, rate 60, PIP 36 cmH2O, FiO2 1.00 and PEEP 5 cmH2O. ABG results on these settings were: pH 7.34, PCO2 44 mmHg and PO2 46 mmHg.
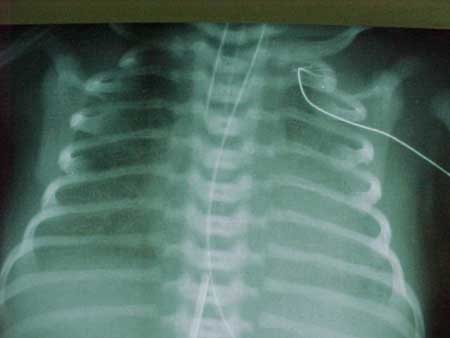
The chest x-ray (CXR) (Figure 1) showed no improvement.

Due to the high PIP required with little improvement in oxygenation, the decision was made to place the infant on High Frequency Oscillation (HFO). Mean airway pressure was titrated to achieve SpO2 100%. Settings on HFO were: 10 Hz, Mean Paw 24.5 cmH2O, Delta P 42 cmH2O and FiO2 1.00. ABG results on these settings were: pH 7.42, PCO2 40 mmHg and PO2 94 mmHg.
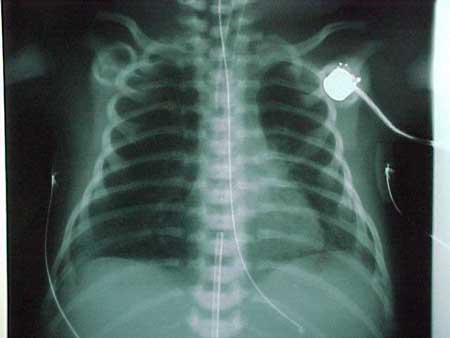
The subsequent CXR (Figure 2) showed adequate inflation to T-9 (9th rib). The endotrachial tube showed high placement and was advanced 2 cm.
Over the next few hours oxygenation remained stable with SpO2 remaining at 100%. A repeat CXR (Figure 3) now showed hyperinflation to T-10 with flattened diaphragms. ABG results were: pH 7.57, PCO2 24 mmHg and PO2 267 mmHg.
Mean Paw was slowly weaned over the next few hours without loss of oxygenation and was now at 23 cmH2O. A repeat CXR (Figure 4) was obtained showing lung inflation back to T-9. Delta P was also weaned during this time and was now 34 cmH2O.
|

Over the next 2 days mean Paw, delta P and FiO2 continued to be weaned successfully. With the infant down to a mean Paw of 14 cmH2O, delta P 22 cmH2O and FiO2 0.30, the infant was returned to conventional ventilation on a Servo 300 on the following settings: SIMV mode, rate 40, PIP 25 cmH2O, FiO2 0.30, PEEP 5 cmH2O and Pressure Support 8 cmH2O. ABG results for these settings were: pH 7.51, PCO2 30 mmHg and PO2 125 mmHg.
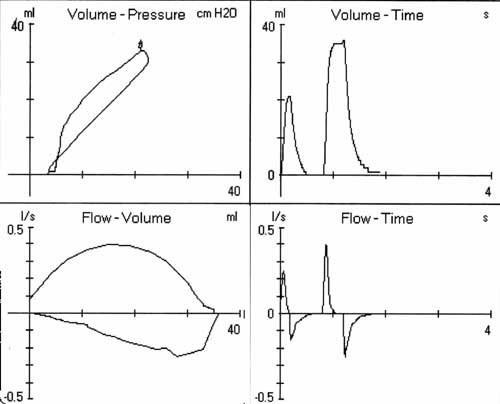
Conventional ventilator settings were weaned over the next day and a half. FiO2 was now at room air with ventilator settings: SIMV mode, rate 15, PIP 19 cmH2O, PEEP 5 cmH2O and Pressure Support 8 cmH2O. Ventilator waveforms (Figure 5 below) show good compliance. The infant was successfully extubated.
FURTHER READING
- Kinsella JP, Truog WE, Walsh WF, et.al. Randomized, multicenter trial of inhaled nitric oxide and high-frequency oscillatory ventilation in severe, persistent pulmonary hypertension of the newborn. J Pediatr 1997 Jul;131(1 Pt 1):55-62. Considerations. 1998. Armonk, NY, Futura Publishing Company, Inc.
- Kinsella JP, Abman SH. High-frquency oscillatory ventilation augments the response to inhaled nitric oxide in persistent pulmonary hypertension of the newborn: Nitric Oxide Study Group. Chest 1998 Jul;114(1 Suppl):100S
- Donn SB. Neonatal and Pediatric Pulmonary Graphics: Principles and Clinical Considerations. 1998. Armonk, NY, Futura Publishing Company, Inc.
DISCUSSION:
Do you think the staff recognized and managed the case appropriately? Post your thoughts or ask other questions related to this case.